













Quick Answer
The Department of Veterans Affairs (VA) rates sleep apnea based on its severity and the treatment required, ranging from 0% to 100% disability. A 50% rating may be assigned to veterans who require a Continuous Positive Airway Pressure (CPAP) machine or similar breathing assistance device. Understanding the VA’s criteria, which consider factors like diagnostic findings and treatment necessity, is essential for a successful VA disability claim.
Why This Update
Over a million veterans are rated for sleep apnea, but many more are either underrated or haven’t filed at all. We built this guide to walk you through the exact rating criteria, evidence requirements, and claim strategies so nothing gets left on the table.
Author’s Take
Sleep apnea is one of the most common conditions I see veterans struggle to get rated — not because they don’t have it, but because they don’t know how to prove the connection to their service. The biggest mistake? Filing without a nexus letter or relying on a home sleep test instead of a full sleep study. If you’re using a CPAP every night, you may qualify for a 50% rating. But the VA needs to see the right evidence laid out clearly. My advice: get a proper sleep study, ask your doctor for a detailed nexus letter, and don’t overlook the secondary connection route — especially if you’re already rated for PTSD or chronic pain.
How Does the VA Rate Sleep Apnea in 2026?
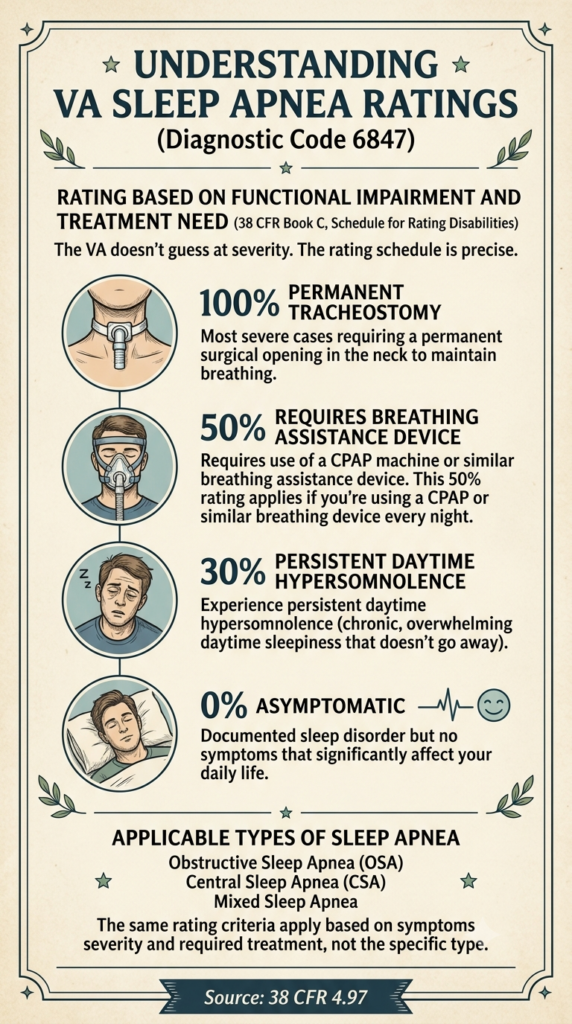
The VA rates sleep apnea under diagnostic code 6847 of the 38 CFR Book C, Schedule for Rating Disabilities, within the respiratory system. The VA doesn’t guess at severity. The rating schedule is precise and based on how the condition affects you and what treatment you need.
The VA Schedule for Rating Disabilities under diagnostic code 6847 (Sleep Apnea Syndromes) provides ratings of 0% for asymptomatic, 30% for persistent daytime hypersomnolence, 50% for requiring a CPAP machine, and 100% for permanent tracheostomy, as detailed in 38 CFR 4.97. A 50% rating applies when the condition requires a CPAP machine or similar breathing assistance device. If you’re using a CPAP or similar breathing device every night, that’s the threshold you’ve met.
The 0% rating applies when you have a documented sleep disorder but no symptoms that significantly affect your daily life. The 30% rating applies when you experience persistent daytime hypersomnolence (chronic, overwhelming daytime sleepiness that doesn’t go away). The 100% rating is reserved for the most severe cases requiring a permanent tracheostomy, a surgical opening in the neck to maintain breathing.
The VA considers various forms of sleep apnea, including Obstructive Sleep Apnea (OSA), Central Sleep Apnea (CSA), and Mixed Sleep Apnea. It applies the same rating criteria based on functional impairment. What matters isn’t the specific type you have. It’s how severe your symptoms are and what treatment you need to manage them.
What are the Types of Sleep Apnea and Their Impact on VA Ratings?
Obstructive Sleep Apnea (OSA) is the most common form, marked by repeated episodes of complete or partial airway obstruction during sleep. Your airway physically collapses or becomes blocked, cutting off breathing repeatedly throughout the night. This is what most veterans deal with, and it’s often linked to weight gain, aging, or anatomical factors.
Central Sleep Apnea (CSA) occurs when the brain fails to send proper signals to the muscles that control breathing. This leads to periods of no breathing. This isn’t a physical blockage—it’s a neurological issue. CSA is less common but can be connected to service-related traumatic brain injuries or other neurological conditions.
Mixed Sleep Apnea combines features of both OSA and CSA, which makes diagnosis and treatment more complex. You might start the night with obstructive episodes and shift to central apnea patterns later, or vice versa. It’s harder to manage and often requires more sophisticated treatment approaches.
The VA rating schedule focuses on the functional impact and required treatment, not solely on the specific diagnostic subtype. Whether your sleep apnea is obstructive, central, or mixed, the VA applies the same rating criteria. What they care about is whether you need a CPAP, whether you’re chronically exhausted during the day, or whether your condition is severe enough to require surgery.
How Do Veterans Establish Service Connection for Sleep Apnea?
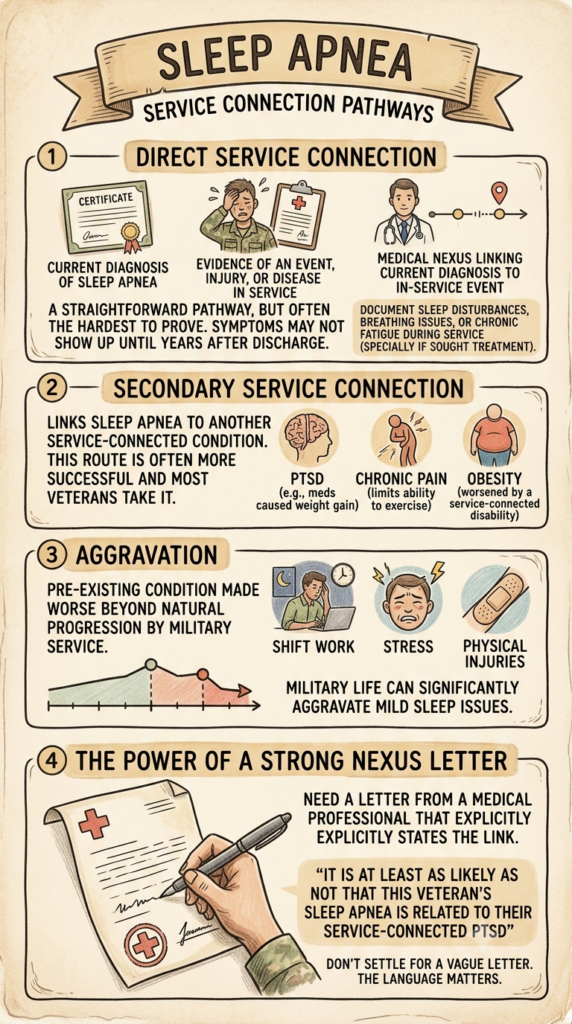
Direct service connection requires three elements: a current diagnosis of sleep apnea, evidence of an event, injury, or disease in service, and a medical nexus linking the current diagnosis to the in-service event. This is the straightforward path. But it’s often the hardest to prove for sleep apnea because symptoms may not show up until years after discharge.
If you can document sleep disturbances, breathing issues, or chronic fatigue during your service (especially if you sought treatment for them), that’s your in-service event. Then you need a doctor to connect the dots between what happened during service and your current diagnosis. That’s where the nexus letter comes in.
Secondary service connection links sleep apnea to another service-connected condition, such as PTSD, chronic pain, or obesity worsened by a service-connected disability. This is the route most veterans take, and it’s often more successful. If you’re already rated for PTSD and your psychiatrist has you on medications that caused weight gain, or if your chronic pain limits your ability to exercise, those can be legitimate pathways to secondary service connection for sleep apnea.
Aggravation occurs when a pre-existing sleep apnea condition is made worse beyond its natural progression by military service, which may qualify for service connection. Even if you had mild sleep issues before service, if military life (shift work, stress, physical injuries) made it significantly worse, you may qualify.
You need a strong nexus letter from a medical professional that explicitly states the link between service and sleep apnea. Don’t settle for a vague letter. You need a doctor who will say, clearly and specifically, “It is at least as likely as not that this veteran’s sleep apnea is related to their service-connected PTSD” or whatever the connection is. That language matters.
What Medical Evidence is Essential for a Strong VA Sleep Apnea Claim?
A polysomnography (sleep study) is the gold standard for diagnosing sleep apnea. Include it as evidence. This should be a full, attended sleep study if possible. Home sleep tests can work, but an in-lab study provides more complete data and carries more weight with the VA. The study will measure your apnea-hypopnea index (AHI), oxygen levels, and sleep disruptions—all the metrics the VA uses to confirm your diagnosis.
You need detailed medical records from a physician: symptom complaints, diagnostic findings, and the prescribed treatment plan (CPAP prescription and compliance data). If you’ve been using a CPAP, get the compliance data from your machine. The VA wants to see that you’re actually using the device as prescribed. That proves the severity and ongoing nature of your condition.
Lay statements from you and supporting statements from family or friends can provide credible evidence of when the condition started and how it affects daily life. Your spouse can write about how your snoring has worsened, how you stop breathing at night, or how exhausted you are during the day. Your buddy from your unit can describe how you were always falling asleep during downtime or struggling with fatigue. These statements fill in gaps that medical records can’t.
A detailed nexus letter from a doctor or medical expert is often critical, especially for secondary claims or claims where direct service connection isn’t immediately clear. Find a doctor who understands VA claims and can write a detailed, evidence-based opinion. Generic letters don’t cut it. You need specifics: the medical research linking PTSD to sleep apnea, the timeline of your symptoms, and a clear statement that your service caused or worsened your condition.
Can Sleep Apnea Ratings Be Increased or Appealed?
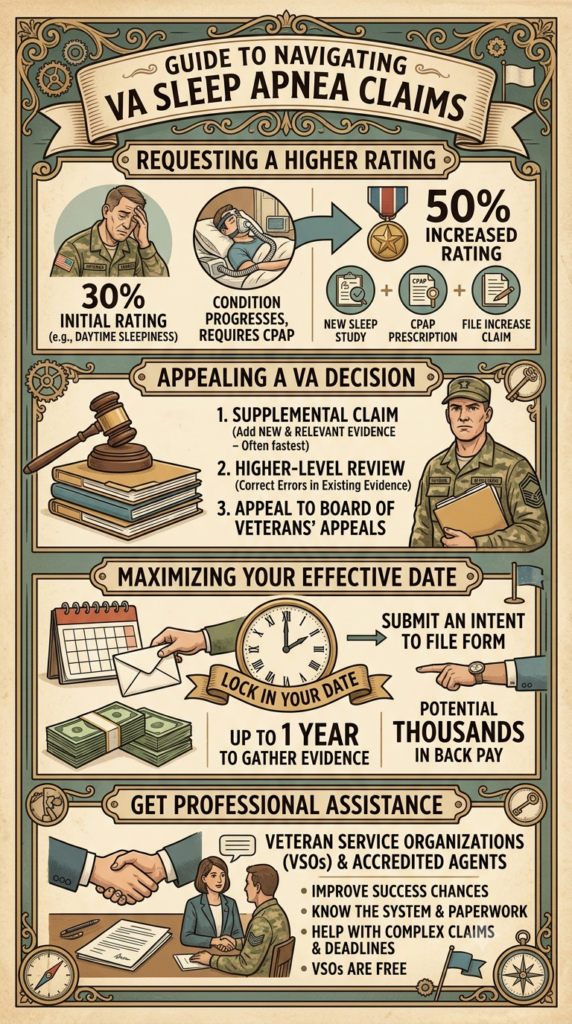
If your sleep apnea worsens, or if you go from not needing a CPAP to requiring one, you can file for an increased rating based on updated medical evidence. Let’s say you were initially rated at 30% for daytime sleepiness, but your condition progressed and now you need a CPAP. That’s a clear path to a 50% rating. Get a new sleep study, document the CPAP prescription and usage, and file the increase claim.
Veterans can appeal an unfavorable initial decision through several avenues: filing a Supplemental Claim with new and relevant evidence, requesting a Higher-Level Review, or appealing to the Board of Veterans’ Appeals. If the VA denied your claim or gave you a lower rating than you expected, don’t assume it’s over. The Supplemental Claim route is often the fastest if you have new medical evidence. A Higher-Level Review works if you think the VA made an error interpreting the evidence you already submitted.
The effective date of a claim is important because it determines when benefits can begin. It’s usually tied to the date the VA received the claim or intent to file. If you’re thinking about filing but aren’t ready yet, submit an Intent to File form. That locks in your potential effective date for up to a year while you gather evidence. It can mean thousands of dollars in back pay.
Getting help from a Veteran Service Organization (VSO) or an accredited claims agent can improve your chances of a successful appeal or increased rating. VSOs are free, they know the system, and they can help you work through the paperwork and deadlines. If your claim is complex or you’ve been denied multiple times, it’s worth getting professional help.
Example Scenario
If you are a veteran who served in a high-stress environment and later developed symptoms consistent with sleep apnea, getting a formal diagnosis through a sleep study is the first critical step. Even if your symptoms emerged years after service, collecting medical evidence and getting a detailed nexus letter from your doctor that explicitly links your sleep apnea to service-related stressors, injuries, or another service-connected condition can strengthen your VA disability claim. This approach helps the VA understand the full impact of your service on your health.
Frequently Asked Questions
What is the most common VA rating for sleep apnea?
The most common VA rating for sleep apnea is 50%, typically awarded to veterans who require a Continuous Positive Airway Pressure (CPAP) machine or other assistive breathing devices for treatment.
Can I get a 100% VA rating for sleep apnea?
Yes, a 100% VA rating for sleep apnea is possible, but it is reserved for the most severe cases where the condition requires a permanent tracheostomy, a surgical procedure to create an opening in the neck for breathing.
Is sleep apnea considered a presumptive condition by the VA?
No, sleep apnea is generally not considered a presumptive service-connected condition by the VA for most veterans. However, specific circumstances, such as a link to certain environmental exposures or a secondary connection to another service-connected presumptive condition, might allow for presumptive consideration.
How do I prove service connection for sleep apnea if I was diagnosed after service?
To prove service connection for a post-service diagnosis, you need a current diagnosis, evidence of an in-service event or condition (or aggravation of a pre-existing one), and a medical nexus letter from a doctor linking the two. Secondary service connection is also a common pathway.
Can sleep apnea be service-connected secondary to other conditions like PTSD?
Yes, sleep apnea can often be service-connected secondary to other service-connected conditions, particularly those that contribute to weight gain (like some medications for mental health conditions) or alter upper airway anatomy, such as PTSD or chronic pain.
What happens if my sleep apnea worsens after I receive a VA rating?
If your sleep apnea worsens, or if your treatment needs change (e.g., you now require a CPAP when you previously didn’t), you can file a claim for an increased rating with the VA, providing updated medical evidence to support the increased severity.
 AllVeteran.com Advisors
AllVeteran.com Advisors
With expertise spanning local, state, and federal benefit programs, our team is dedicated to guiding individuals towards the perfect program tailored to their unique circumstances.




